The Tumor That Can Affect Hearing
Understanding Acoustic Neuroma
Updated December 2025
If you've noticed a shift in your hearing — particularly in one ear, and ringing or buzzing in that ear (tinnitus) — it could be your body's way of communicating something important.
Although extremely rare, something to be aware of is acoustic neuroma. Affecting about 3,000 people in the United States each year, this noncancerous tumor grows on the lining of the eighth cranial nerve (there are 12 total), which connects the ear to the brain. The eighth cranial nerve, also known as the vestibulocochlear nerve, plays a vital role in your hearing and balance. A tumor can get in the way of its function.
We tailor treatment to preserve as much hearing as possible.— Richard M. Wiet, MD
"Anyone can develop this type of inner-ear tumor, but they typically occur in adults between the ages of 50 and 60," says R. Mark Wiet, MD, a neuro-otologist and lateral skull base surgeon who leads the Northwestern Medicine Acoustic Neuroma Program. This multidisciplinary program brings together specialists in neurotology, neurosurgery, radiation oncology, neuro-oncology, neuroradiology, audiology and physical therapy who have expertise in diagnosing and treating this rare condition.
The lining of the cranial nerve is made up of Schwann cells, which support and protect nerves. Dr. Wiet likens the cranial nerve to a power cord. "The Schwann cells are the protective plastic on the outside of the cord," he says. "This outer part is where an acoustic neuroma will form."
What Are the Symptoms?
While not everyone who has an acoustic neuroma experiences symptoms, these two are the most common, according to Dr. Wiet:
- Hearing loss, usually starting gradually in one ear
- Tinnitus, ringing or buzzing in the affected ear
Dizziness, balance problems and headaches can also be associated with acoustic neuromas, but are less common. Large tumors can press on nearby facial nerves, which can create facial numbness or paralysis. It is important to note that all of these symptoms can occur from other conditions. If you are experiencing any of them, talk with your physician.
Acoustic Neuroma Risk Factors
The cause of most acoustic neuromas is not known, and there is no current evidence that environmental factors such as smoking or cellphone use increase the risk of developing this type of tumor. In about 5% of cases, an acoustic neuroma has been associated with a genetic condition called neurofibromatosis type 2 (NF2). NF2 predisposes people to develop tumors in the nerves of their head and spinal cord.
While the inciting factor for acoustic neuromas remains unknown, what is known is that something causes a gene on chromosome 22 to malfunction. "That gene is for a protein called merlin, which is like a governor protein that controls the growth of Schwann cells," explains Dr. Wiet. "This lack of control of growth is where the problem arises."
Most acoustic neuromas grow slowly, at a rate of about 1 to 2 millimeters per year, and do not spread throughout the body. They also do not invade the brain, but they can push on the brain as they grow.
Acoustic neuromas are often described in sizes:
- Small (less than 2 centimeters [cm])
- Medium (2 to 4 cm)
- Large (more than 4 cm)
Next Steps: Diagnosis and Treatment
Diagnosis of acoustic neuromas usually starts with a hearing test called an audiogram, followed by magnetic resonance imaging (MRI) of the head and inner ears.
Treatment options depend on the size and location of the tumor, your age and health, as well as the severity of your symptoms. "Personal preference is also taken into consideration," says Dr. Wiet. "We consider the natural course of the disease and prioritize not introducing any other symptoms from the treatment." Treatment options include:
- Observation: If your tumor is small and not causing significant problems, monitoring may be sufficient. "I've had patients in observation for 20 years who do not need any further treatment," explains Dr. Wiet. "We check these patients more frequently at first and then over time, if their tumor is not growing, we start decreasing the frequency of their MRIs."
- Traditional surgery: Removing all or part of an acoustic neuroma, either through your ear or through a flap in your skull, is more commonly used to treat larger tumors or tumors that are causing concerning symptoms. Traditional surgery is typically a better choice for younger patients who can tolerate anesthesia, surgery and recovery.
- Stereotactic radiosurgery: This minimally invasive procedure uses focused radiation beams to damage the DNA within tumor cells, stopping their ability to divide. It's used more frequently on small- to medium-sized tumors, and in older adults who cannot tolerate surgery for health reasons.
"In general, people do well with treatment as long as they're in experienced hands," says Dr. Wiet. "When surgery is the preferred treatment, the goal is total tumor removal. However, occasionally we will leave a small amount of tumor behind if it is densely adherent to important cranial nerves, blood vessels, or the brainstem."
Managing Hearing Loss
"At Northwestern Medicine, we tailor treatment to preserve as much hearing as possible," says Dr. Wiet. "However, while living with an acoustic neuroma and after treatment, some patients can experience hearing loss." If hearing loss is a side effect that you might be facing or experiencing, talk with your care team about the possibility of hearing restoration. This can include:
- Traditional hearing aids
- Bone-anchored hearing aids
- Contralateral routing of signal (CROS) hearing aids
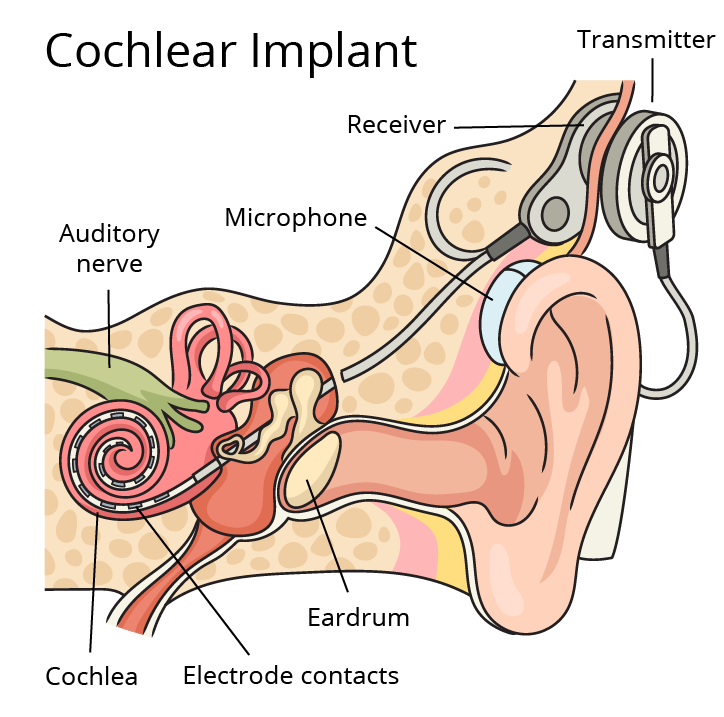
- Cochlear implants
Your care team can help you decide what's right for you.
Featured Experts